Blog
Clinical evidence insights, methodology deep-dives, and the latest in clinical decision support from the Ailva team.
KDIGO 2026 CKD Guidelines: Key Updates for Nephrology Practice
The 2026 KDIGO guidelines introduce significant changes to CKD staging, SGLT2 inhibitor recommendations, and GLP-1 agonist integration. Here is what changed and what it means for your patients.

SGLT2 Inhibitors in Heart Failure: Evidence, Dosing, and Clinical Decision Points
DAPA-HF and EMPEROR-Reduced established SGLT2 inhibitors as foundational HFrEF therapy. DELIVER and EMPEROR-Preserved extended the benefit to HFpEF. Here is the trial-by-trial evidence and practical prescribing guidance for your heart failure patients.

Immunotherapy Checkpoint Inhibitors: A Clinical Guide for Oncologists
PD-1, PD-L1, and CTLA-4 inhibitors have transformed solid tumor oncology. This guide covers approved indications, biomarker selection, immune-related adverse event management, and combination strategies across major tumor types.

Sepsis Management: From Early Recognition to Evidence-Based Resuscitation
The Surviving Sepsis Campaign 2024 guidelines refined the approach to sepsis resuscitation, antibiotic timing, and vasopressor selection. This review covers the current evidence for hour-1 bundle compliance, fluid strategy, and organ support.

Treatment-Resistant Depression: Augmentation Strategies and Emerging Therapies
One-third of patients with major depressive disorder do not respond to first-line antidepressants. This review covers evidence-based augmentation strategies including lithium, atypical antipsychotics, ketamine/esketamine, and psilocybin-assisted therapy.

Type 2 Diabetes Management 2026: ADA Standards of Care Updates
The 2026 ADA Standards of Care introduce updated guidance on GLP-1 agonist and GLP-1/GIP dual agonist positioning, cardiovascular risk reduction, and technology-assisted management. Key changes for primary care and endocrinology practice.

Alzheimer's Disease Treatment 2026: Anti-Amyloid Antibodies and Beyond
Lecanemab and donanemab demonstrated meaningful clinical benefit in amyloid-positive early Alzheimer's disease. This review covers the evidence, ARIA monitoring, patient selection criteria, and the emerging treatment landscape for neurologists and primary care physicians.

GOLD 2026 COPD Guidelines: Triple Therapy, Biologics, and Exacerbation Prevention
The 2026 GOLD report updates the COPD management framework with revised ABCD grouping, expanded triple therapy recommendations, and emerging biologic therapies for eosinophilic COPD. A practical guide for pulmonologists and primary care.

JAK Inhibitor Safety in Rheumatology: Navigating the ORAL Surveillance Aftermath
The ORAL Surveillance trial raised cardiovascular and malignancy concerns for JAK inhibitors in RA. This review examines the current safety landscape, appropriate patient selection, and how to position JAK inhibitors in the rheumatologic treatment algorithm.

MASH (Metabolic-Associated Steatohepatitis): The New Treatment Landscape
With resmetirom (Rezdiffra) becoming the first FDA-approved therapy for MASH in 2024, the treatment paradigm has shifted fundamentally. This guide covers the evidence, patient selection, and the pipeline of emerging therapies for gastroenterologists and hepatologists.

Antibiotic Stewardship 2026: Resistance Trends and Empiric Therapy Updates
Antimicrobial resistance continues to accelerate globally. This review covers updated empiric therapy recommendations, de-escalation strategies, and the role of rapid diagnostics in optimizing antibiotic prescribing for common infectious syndromes.

Atrial Fibrillation: Rate vs Rhythm Control in 2026 — EAST-AFNET 4 and Beyond
EAST-AFNET 4 shifted the paradigm toward early rhythm control in AF, demonstrating a 21% reduction in cardiovascular outcomes. This review examines the evolving evidence for rhythm control strategies, DOAC selection, and catheter ablation outcomes in the context of current guidelines.

Acute Coronary Syndrome: STEMI and NSTEMI Management Updates for 2026
Recent trial data from FIRE, MULTISTARS AMI, and TOMAHAWK have refined revascularization strategy, timing, and antiplatelet selection in ACS. This article reviews the current evidence for complete revascularization, de-escalation antiplatelet therapy, and risk-stratified NSTEMI management.

Thyroid Nodule Evaluation: Bethesda Classification, Molecular Testing, and When to Biopsy
Thyroid nodules are detected in up to 68% of adults on high-resolution ultrasound, yet fewer than 5% harbor malignancy. This review covers the ACR TI-RADS system for biopsy decision-making, Bethesda cytopathology classification, and the role of molecular testing in indeterminate nodules.
Migraine Prevention: CGRP Inhibitors, Comparative Efficacy, and Treatment Selection
CGRP-targeting therapies have transformed migraine prevention, offering the first mechanism-specific preventive class. This review compares the four anti-CGRP monoclonal antibodies and two gepant preventives, covering efficacy data, onset of action, and practical selection for episodic and chronic migraine.

Psoriasis Biologics: IL-17 vs IL-23 Inhibitors in Head-to-Head Trials
Biologic therapy for moderate-to-severe psoriasis now includes multiple IL-17 and IL-23 inhibitors with PASI 90 and PASI 100 rates exceeding 60-80%. This review summarizes head-to-head trial data comparing these mechanisms and guides clinical selection based on efficacy, durability, and safety.

IBD Management: Vedolizumab, Ustekinumab, and JAK Inhibitors in UC and Crohn Disease
The IBD therapeutic landscape has expanded beyond TNF inhibitors to include gut-selective integrins, IL-12/23 blockade, and JAK inhibitors. This review compares positioning, efficacy endpoints, and safety profiles of vedolizumab, ustekinumab, tofacitinib, and upadacitinib in ulcerative colitis and Crohn disease.
Pulmonary Embolism Risk Stratification: PESI, sPESI, and Outpatient Management
Risk stratification drives PE management from thrombolysis in massive PE to outpatient anticoagulation in low-risk PE. This review covers PESI/sPESI scoring, RV dysfunction assessment, the Hestia criteria for outpatient eligibility, and evolving evidence for intermediate-risk PE management.

Chronic Pain Management: Multimodal Non-Opioid Approaches and Evidence Review
Multimodal non-opioid pain management has become the standard of care for chronic non-cancer pain. This review covers the evidence for gabapentinoids, SNRIs, topical agents, interventional procedures, and structured physical rehabilitation, with practical prescribing guidance for primary care and pain specialists.
HIV PrEP and Treatment: Long-Acting Injectable Cabotegravir and Lenacapavir
Long-acting injectable HIV prevention and treatment have transformed adherence paradigms. This review covers cabotegravir for PrEP, lenacapavir as a twice-yearly option, and injectable cabotegravir/rilpivirine for treatment, with efficacy data and practical implementation considerations.

Osteoporosis Pharmacotherapy: Romosozumab, Denosumab, and Sequential Therapy Strategy
The osteoporosis treatment paradigm has shifted from bisphosphonate monotherapy to anabolic-first sequential strategies. This review covers romosozumab efficacy data, denosumab rebound fracture risk, and evidence-based sequencing for high-risk patients.

Pediatric Asthma: Step Therapy Guidelines and Biologic Eligibility Criteria
GINA and NAEPP guidelines define a stepwise approach to pediatric asthma with recent updates incorporating biologics for severe persistent disease. This review covers step therapy from ages 6-17, ICS dosing thresholds, and eligibility criteria for omalizumab, mepolizumab, dupilumab, and tezepelumab.

Gout Management: Treat-to-Target Urate Strategy and IL-1 Inhibitor Therapy
Treat-to-target urate-lowering therapy (ULT) reduces gout flares, tophi burden, and joint damage. This review covers allopurinol dosing optimization, febuxostat cardiovascular safety data, and the role of pegloticase and IL-1 inhibitors in refractory disease.
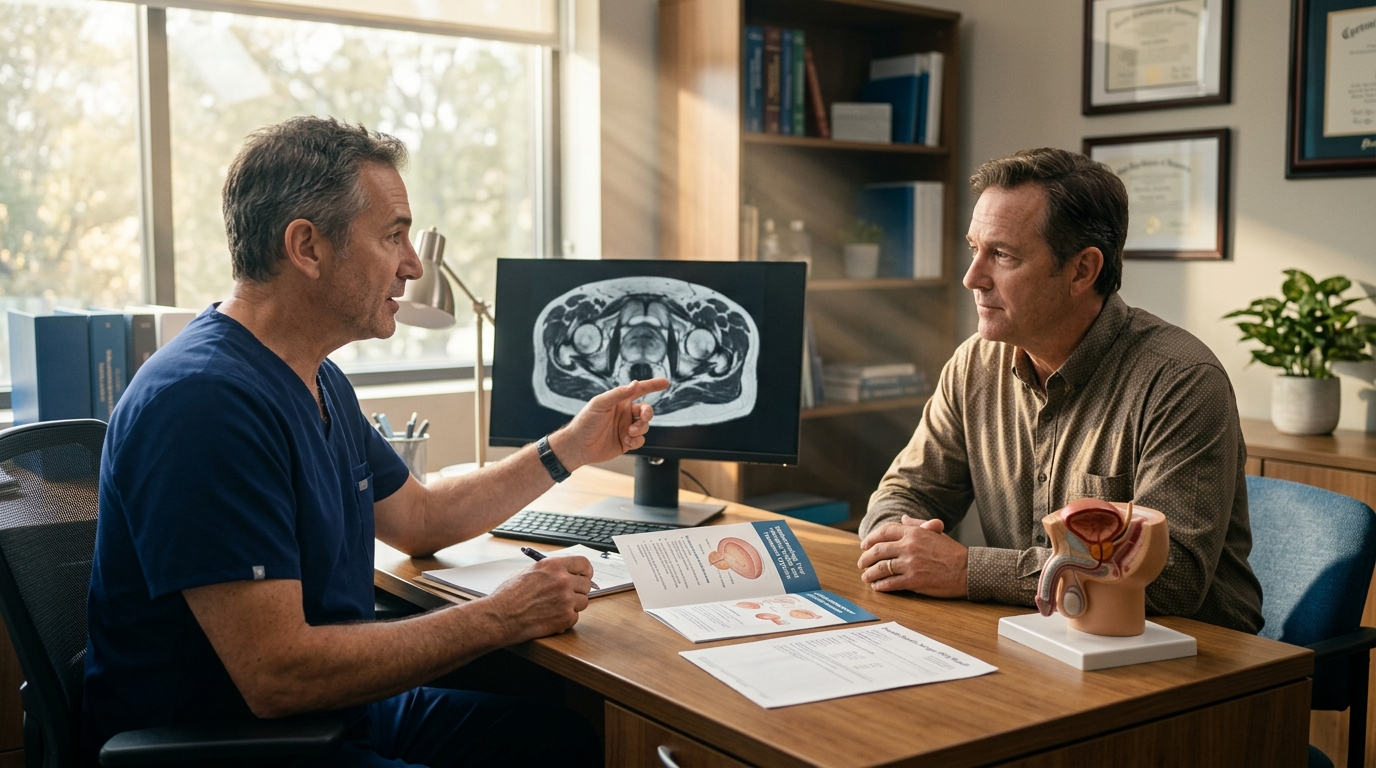
Prostate Cancer Screening: USPSTF Updates, MRI Integration, and Shared Decision-Making
Prostate cancer screening with PSA remains controversial despite updated USPSTF recommendations supporting informed decision-making for men aged 55-69. This review covers the evolving role of prebiopsy MRI, risk calculators, and active surveillance strategies that have changed the risk-benefit calculus.

Peripheral Artery Disease: Revascularization vs Medical Therapy and VOYAGER PAD Data
The BEST-CLI and VOYAGER PAD trials have refined PAD management, clarifying when revascularization improves outcomes and how to optimize antithrombotic therapy post-intervention. This review covers the evidence for medical management versus revascularization, CLTI staging, and dual-pathway inhibition.

Acute Kidney Injury: KDIGO Staging, Prevention Strategies, and Recovery Prediction
AKI affects 10-15% of hospitalized patients and up to 50% of ICU patients, with significant implications for long-term CKD progression and mortality. This review covers KDIGO staging, nephrotoxin stewardship, hemodynamic optimization, and emerging biomarkers for early detection and recovery prediction.
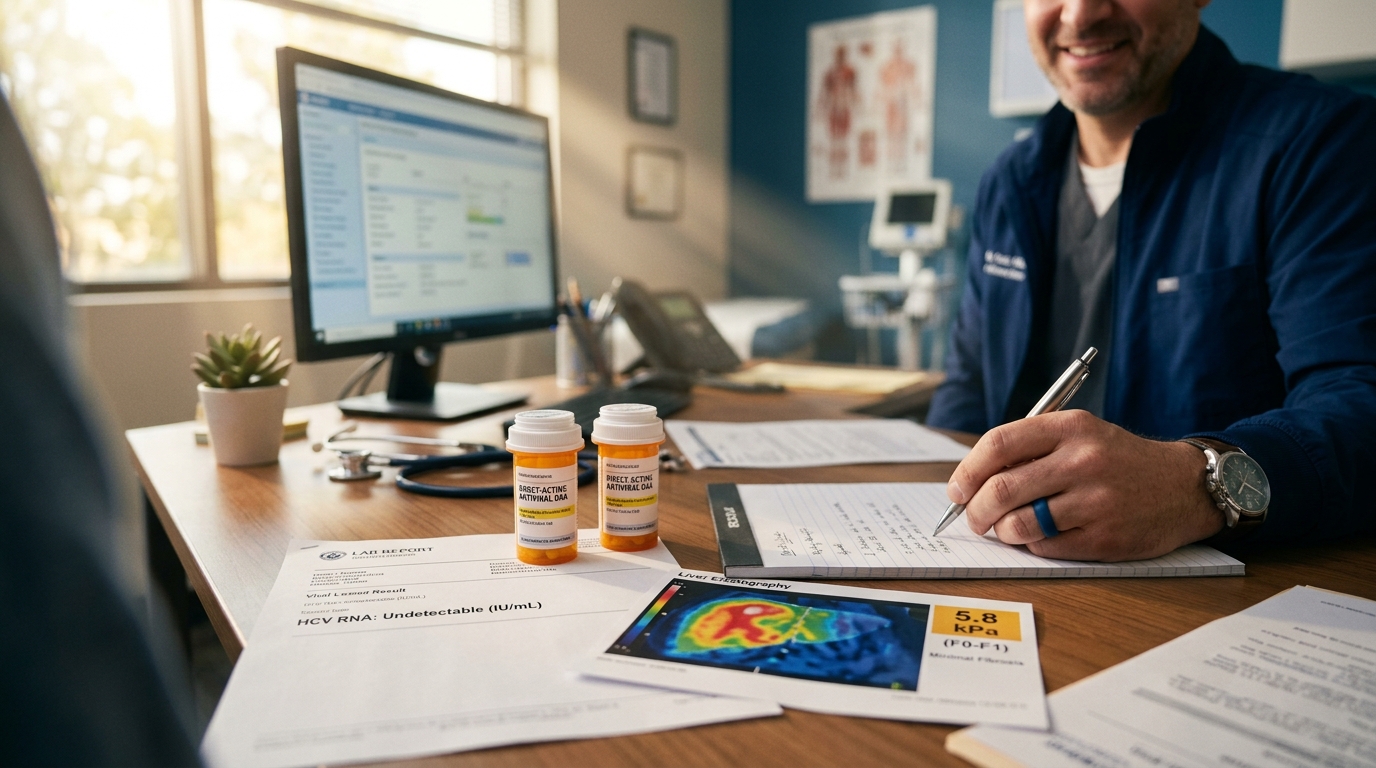
Hepatitis C: Pan-Genotypic DAA Regimens, Treatment Simplification, and Cure Rates
Direct-acting antivirals (DAAs) have transformed hepatitis C into a curable disease with SVR rates exceeding 95% across all genotypes. This review covers current pan-genotypic regimens, treatment simplification for non-cirrhotic patients, and management of decompensated cirrhosis and reinfection.

Venous Thromboembolism Prevention: Post-Surgical and Medical Prophylaxis Strategies
VTE remains a leading cause of preventable hospital death, with 60% of VTE events associated with recent hospitalization. This review covers risk assessment tools, pharmacologic prophylaxis selection, extended thromboprophylaxis after orthopedic surgery and cancer surgery, and the role of DOACs in medical prophylaxis.
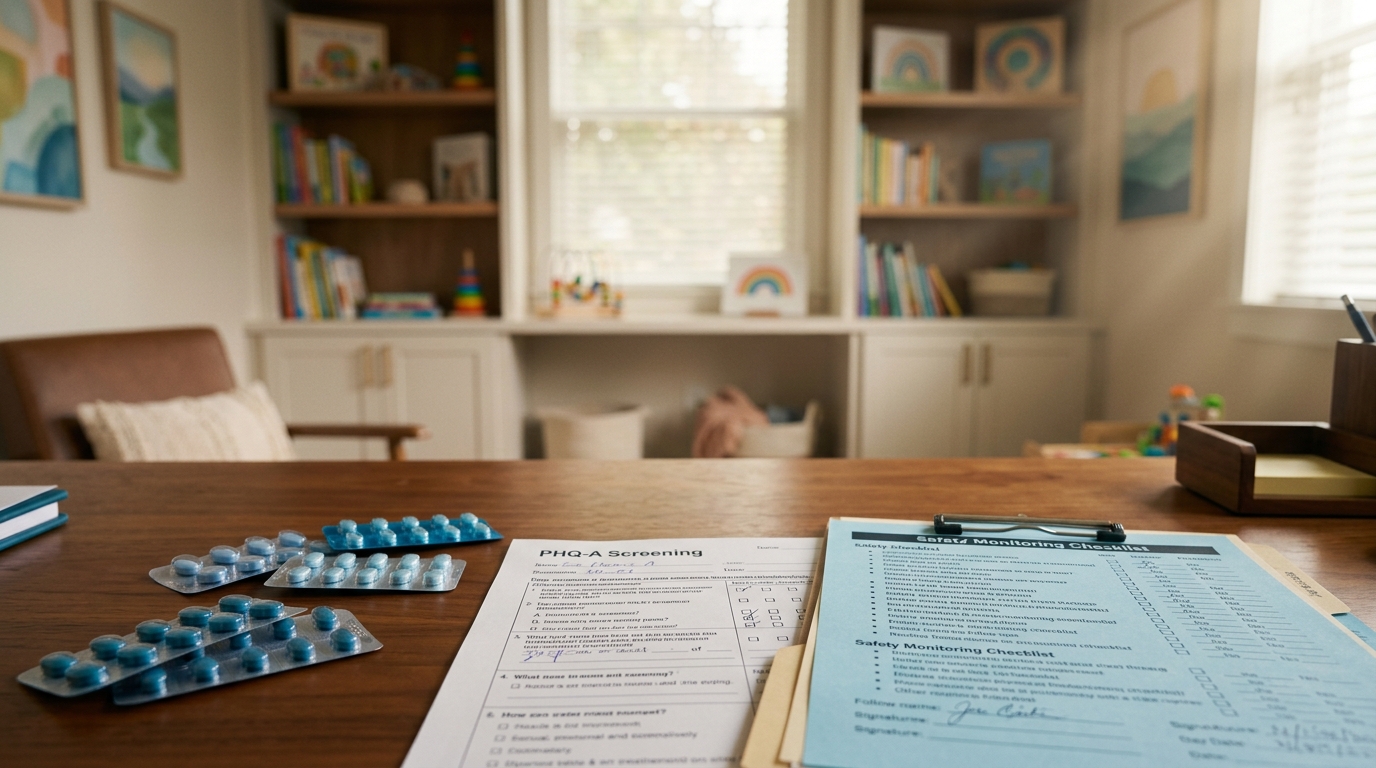
Major Depressive Disorder in Adolescents: SSRI Selection, Monitoring, and Suicidality Risk
Treating adolescent depression requires balancing evidence for SSRI efficacy against the FDA black box warning for suicidality. This review covers first-line SSRI selection, the TADS and TORDIA trial evidence, monitoring protocols, and combination with psychotherapy.
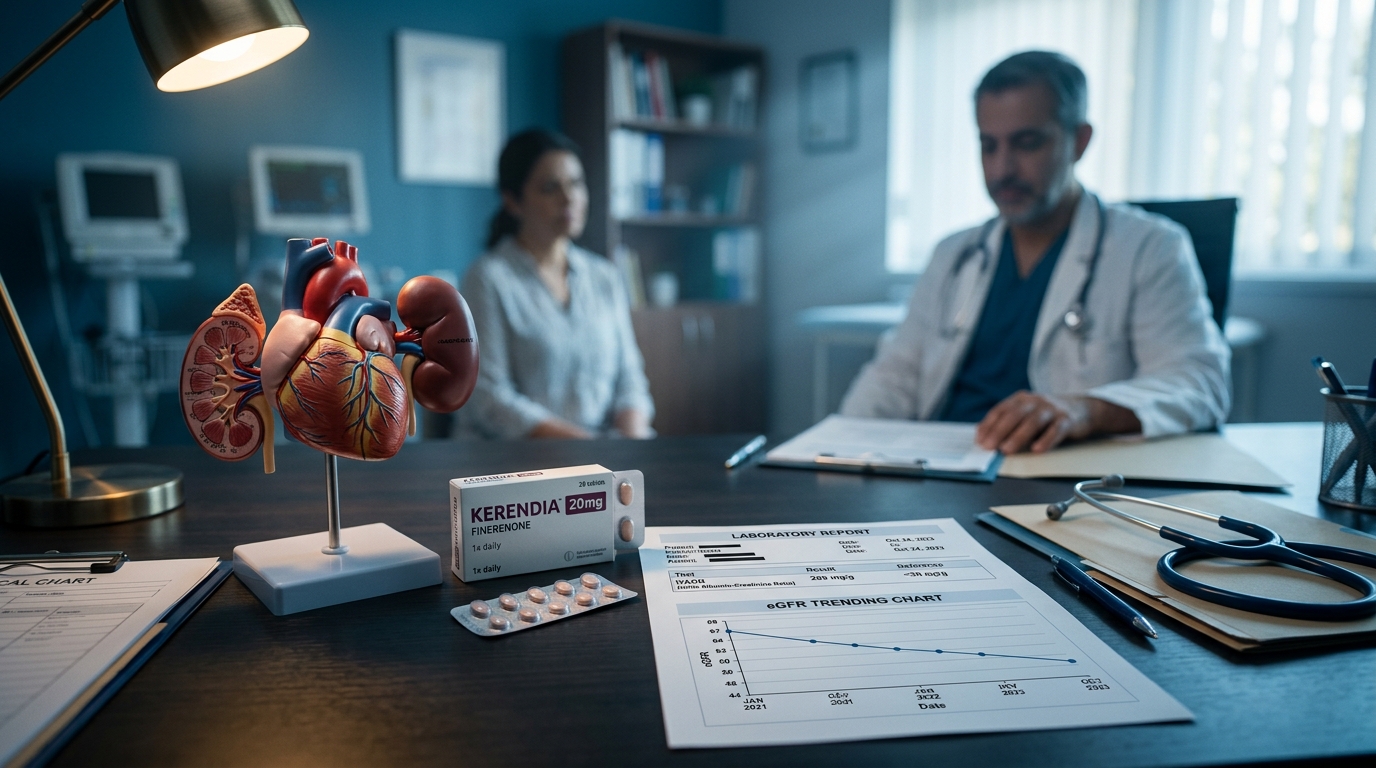
Diabetic Kidney Disease: Finerenone, Nonsteroidal MRAs, and the FIDELIO/FIGARO Evidence
Finerenone, the first nonsteroidal mineralocorticoid receptor antagonist, has demonstrated cardiorenal benefit in DKD beyond SGLT2 inhibitors and RAS blockade. This review covers the FIDELIO-DKD and FIGARO-DKD trials, practical implementation, and the emerging multi-pillar approach to DKD management.

Stroke Prevention: Carotid Stenosis Management and Dual Antiplatelet Therapy Evidence
Management of carotid stenosis and post-stroke antiplatelet strategy have evolved with the CREST-2 and POINT/CHANCE trial data. This review covers the indications for carotid endarterectomy versus stenting, the time-limited dual antiplatelet approach, and the role of intensive medical management.

Clostridioides difficile Infection: Fidaxomicin vs Vancomycin and FMT Evidence
Recurrent C. difficile infection affects 25-35% of patients after initial treatment. This review compares fidaxomicin and vancomycin head-to-head trial data, evaluates tapered-pulsed regimens, and summarizes the pivotal fecal microbiota transplantation evidence including FDA-approved live biotherapeutics.

Hypertension Management: 2026 ACC/AHA Blood Pressure Targets and Treatment Updates
The 2026 ACC/AHA hypertension guidelines refine blood pressure targets and first-line therapy recommendations based on SPRINT, STEP, and ESPRIT trial data. This review provides a practical algorithm for initial drug selection, combination therapy, and resistant hypertension management.
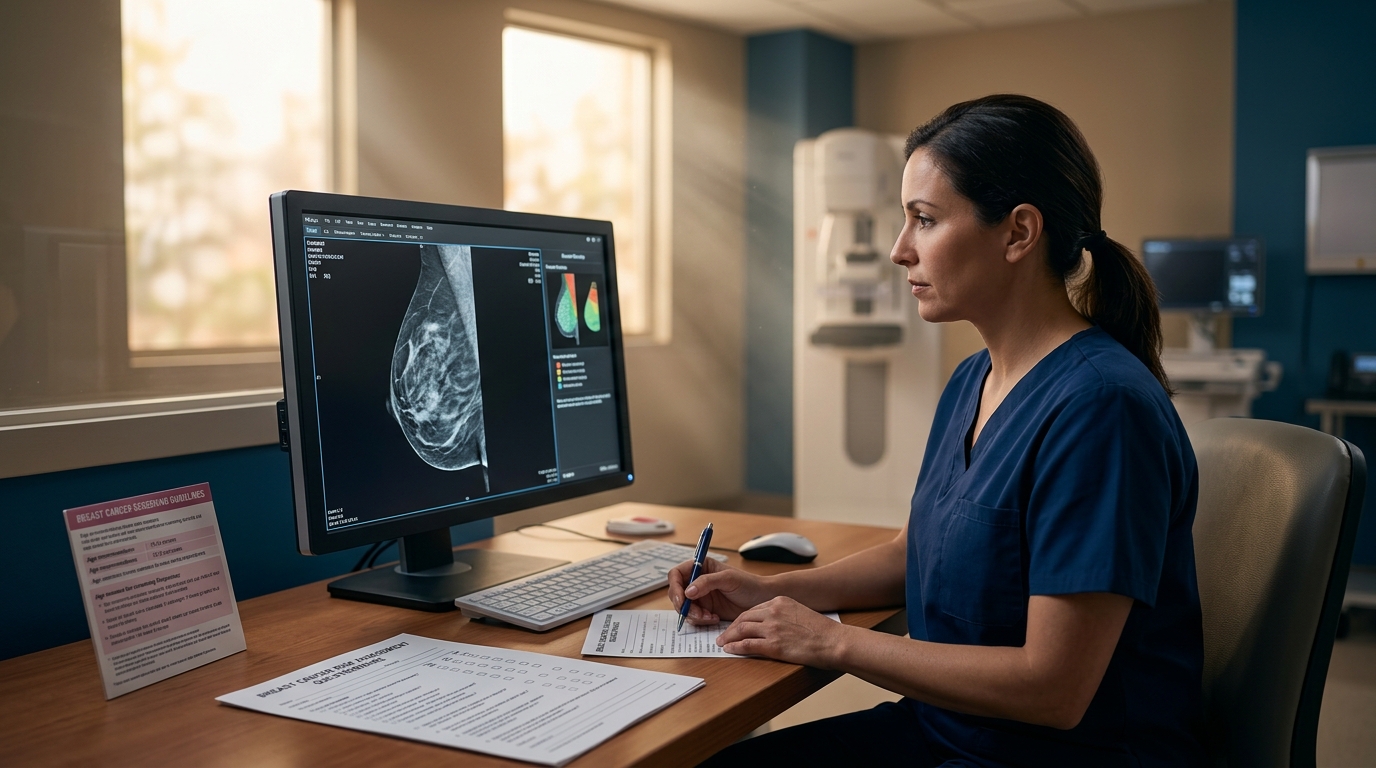
Breast Cancer Screening: Mammography Guidelines and Risk-Based Approaches
Breast cancer screening guidelines diverge across major organizations on starting age, screening interval, and integration of supplemental modalities. This review synthesizes USPSTF, ACS, and ACR recommendations, evaluates risk-stratified screening models, and reviews emerging evidence for contrast-enhanced mammography and abbreviated MRI.

Chronic Heart Failure Monitoring: NT-proBNP Guided Therapy
Natriuretic peptide-guided heart failure management remains debated despite multiple randomized trials. This review evaluates NT-proBNP targets, the GUIDE-IT trial limitations, and practical strategies for incorporating biomarker trends into therapeutic decision-making.

Anaphylaxis Management: Epinephrine Dosing and Biphasic Reactions
Epinephrine remains the only first-line treatment for anaphylaxis, yet it is delayed or withheld in up to 40% of cases. This review covers updated dosing guidelines, optimal route and site of administration, biphasic reaction risk factors, and observation period recommendations.

Cirrhosis Complications: Variceal Bleeding, Ascites, and Hepatic Encephalopathy Management
Decompensated cirrhosis demands systematic management of its life-threatening complications. This review covers current evidence for variceal hemorrhage prophylaxis and treatment, refractory ascites interventions, and hepatic encephalopathy targeting including rifaximin and lactulose protocols.
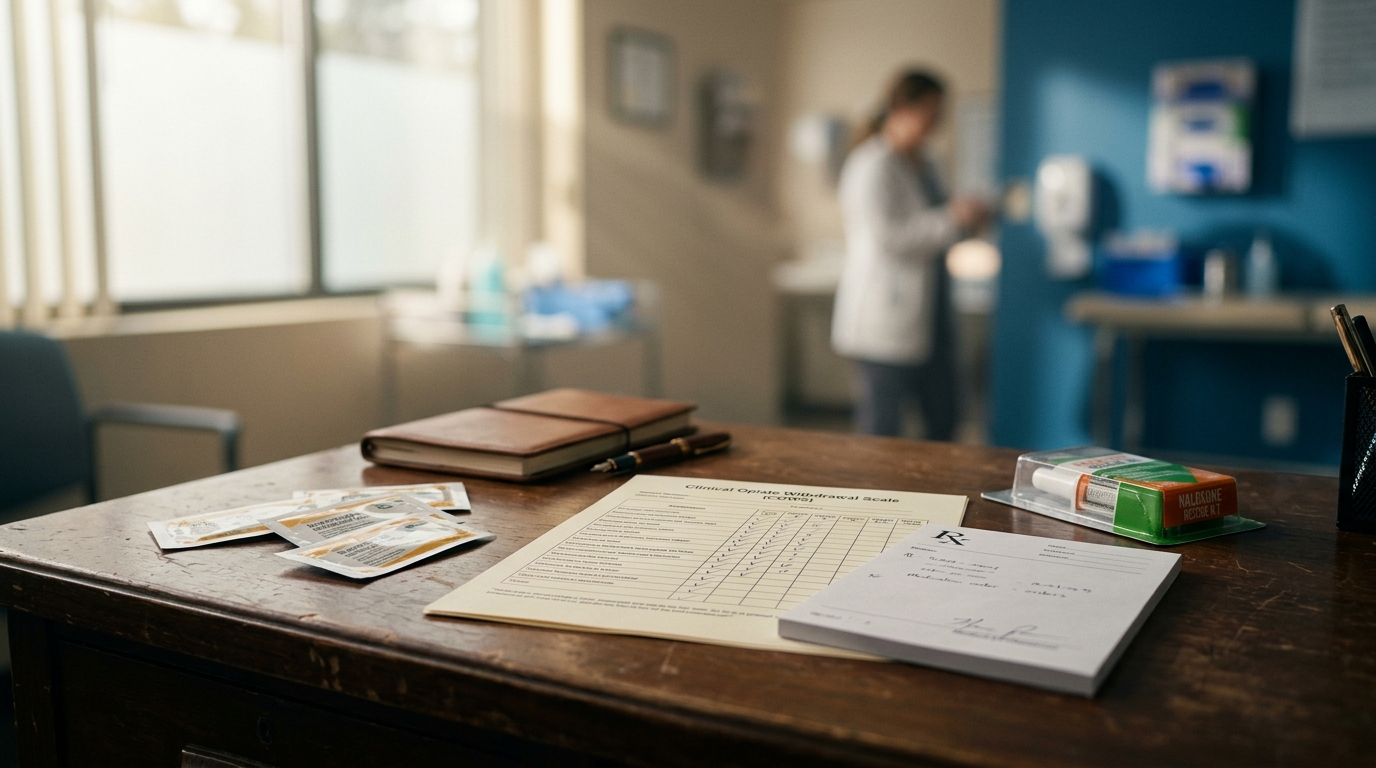
Opioid Use Disorder: Buprenorphine Induction and Maintenance Evidence
Buprenorphine-based medication for opioid use disorder reduces mortality by 50% and is now accessible without the X-waiver in the United States. This review covers induction protocols including low-dose strategies, maintenance dosing, and the evidence for extended-release injectable formulations.

Lung Cancer Screening: LDCT Criteria and Shared Decision-Making
Low-dose computed tomography screening reduces lung cancer mortality by 20-24% in high-risk populations. This review covers the 2024 USPSTF eligibility criteria, Lung-RADS reporting, nodule management algorithms, and strategies for effective shared decision-making in primary care.

Atopic Dermatitis: Dupilumab, JAK Inhibitors, and Emerging Therapies
The treatment landscape for moderate-to-severe atopic dermatitis has expanded dramatically with multiple targeted therapies. This review compares dupilumab, tralokinumab, and JAK inhibitors using pivotal trial data and provides a practical positioning algorithm for dermatologists.

Preeclampsia Prevention and Management: Aspirin Prophylaxis Evidence
Low-dose aspirin prophylaxis reduces preeclampsia risk by 24-62% in high-risk pregnancies when initiated before 16 weeks gestation. This review covers risk stratification, the ASPRE trial findings, optimal dosing, and management of established preeclampsia including magnesium sulfate protocols.

Multiple Sclerosis: Disease-Modifying Therapy Selection Algorithm
The MS treatment landscape now includes over 20 disease-modifying therapies with distinct efficacy, safety, and monitoring profiles. This review provides an evidence-based algorithm for DMT selection in relapsing and progressive MS, incorporating the escalation versus early high-efficacy treatment debate.
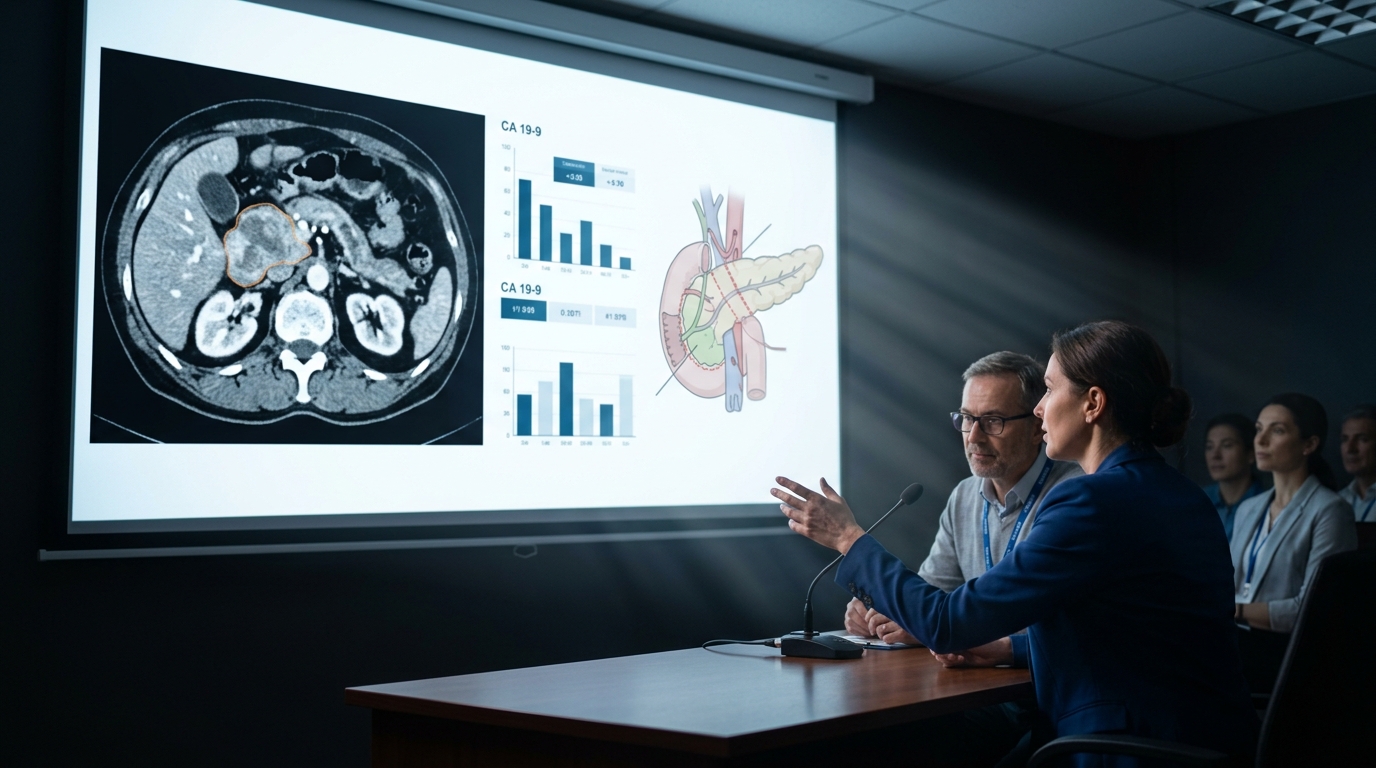
Pancreatic Cancer: Early Detection Biomarkers and Treatment Advances
Pancreatic ductal adenocarcinoma remains the third leading cause of cancer death with a 12% five-year survival rate. This review covers emerging early detection strategies, CA 19-9 limitations, the FOLFIRINOX and gemcitabine/nab-paclitaxel evidence, and emerging immunotherapy approaches.
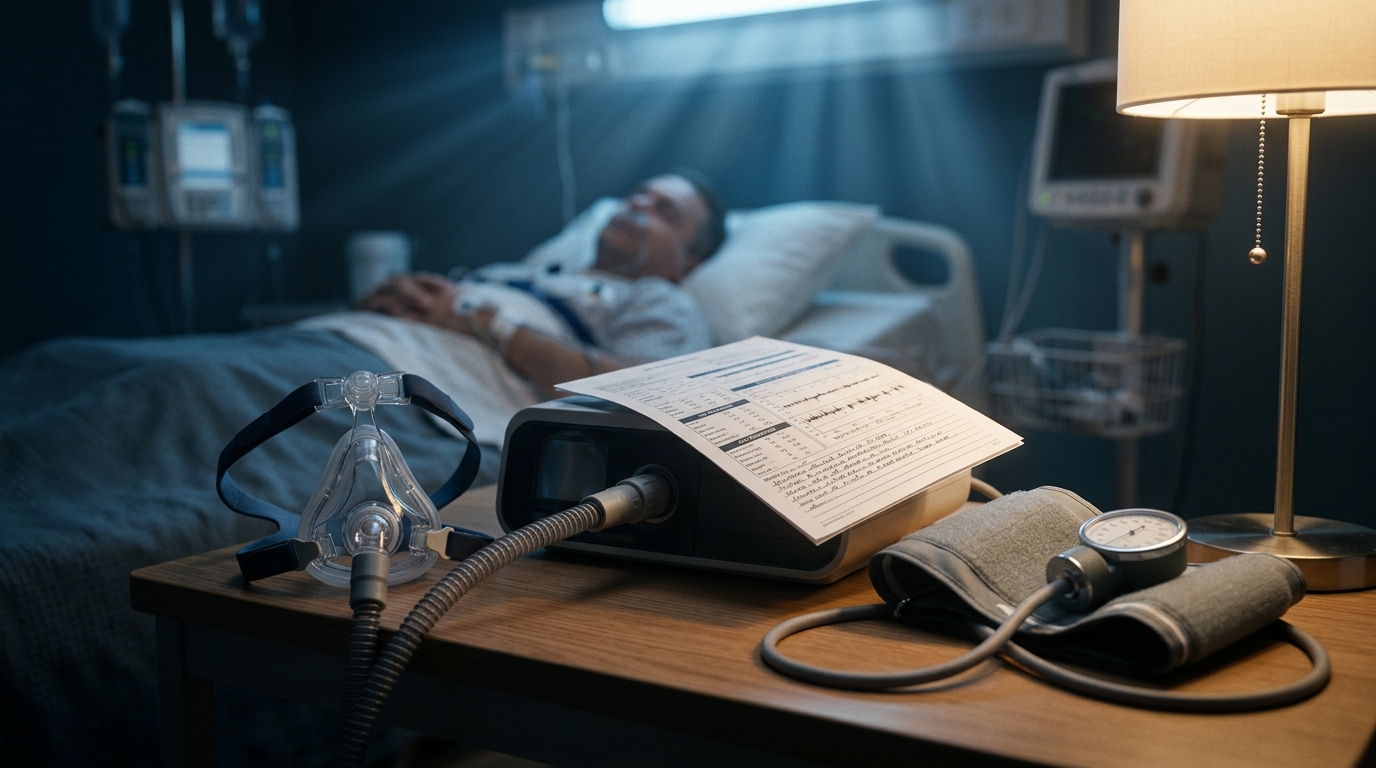
Sleep Apnea and Cardiovascular Risk: CPAP Evidence and Alternatives
Obstructive sleep apnea affects an estimated 1 billion adults globally and is independently associated with hypertension, atrial fibrillation, and heart failure. This review examines the SAVE trial findings on CPAP and cardiovascular outcomes, mandibular advancement devices, and hypoglossal nerve stimulation evidence.

Sickle Cell Disease: Voxelotor, Crizanlizumab, and Gene Therapy
Three novel therapies for sickle cell disease were approved between 2019-2023, and two gene therapies now offer the possibility of functional cure. This review covers voxelotor, crizanlizumab, and L-glutamine evidence, along with the pivotal lovotibeglogene autotemcel and exagamglogene autotemcel data.

Urinary Tract Infections: Antimicrobial Selection and Resistance Patterns
UTI management is complicated by rising fluoroquinolone resistance and ESBL-producing E. coli prevalence. This review covers updated empiric therapy guidelines for uncomplicated cystitis, pyelonephritis, and complicated UTI, with resistance-informed prescribing strategies.

Post-COVID Conditions: Clinical Assessment and Management Framework
Post-COVID conditions affect an estimated 10-20% of SARS-CoV-2 infections and encompass over 200 symptoms across multiple organ systems. This review provides a systematic evaluation framework, evidence-based management strategies, and guidance on differentiating post-COVID from overlapping diagnoses.
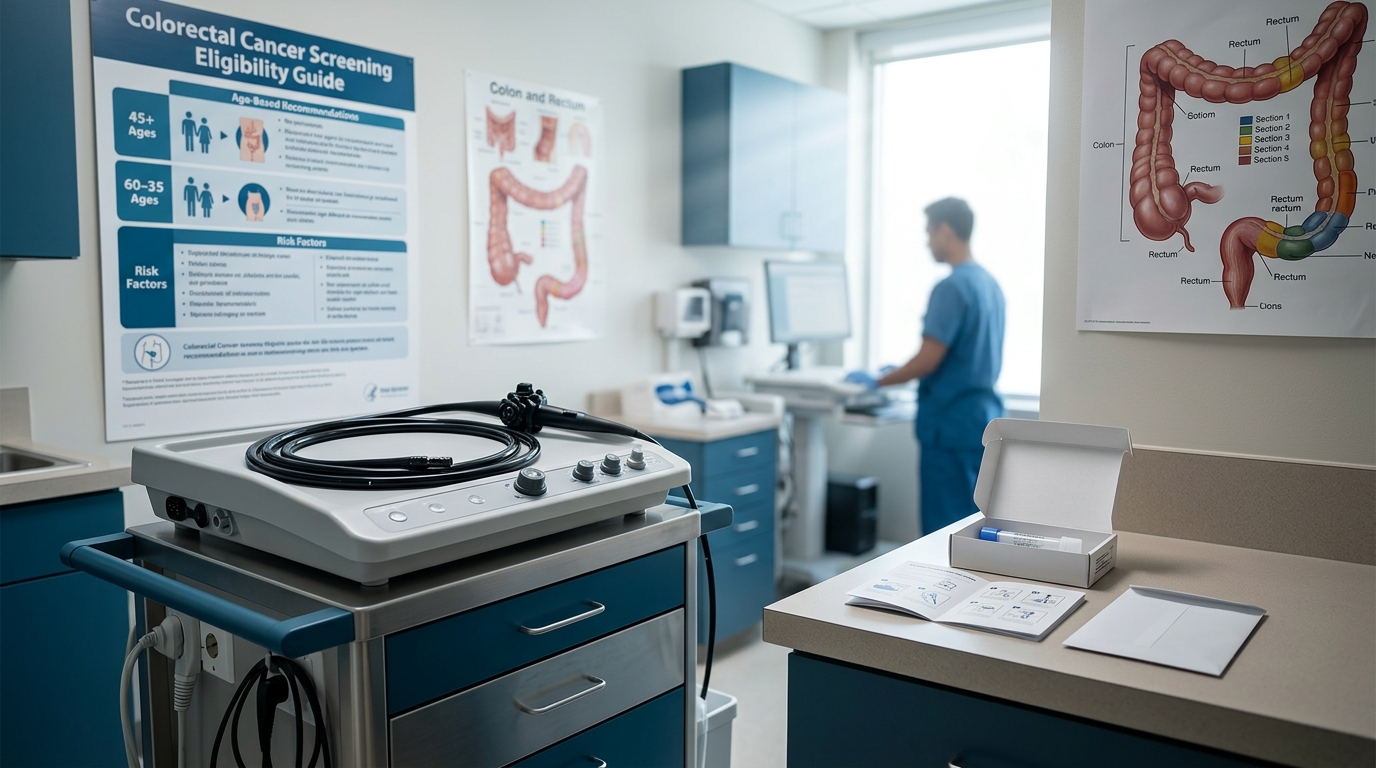
Colorectal Cancer Screening: Age 45 Start and Stool-Based vs Colonoscopy
The lowered screening age to 45 and expansion of stool-based testing options have reshaped the CRC screening landscape. This review compares colonoscopy, FIT, FIT-DNA (Cologuard), and emerging blood-based tests, with guidance on selecting the optimal strategy for individual patients.

Thyroid Cancer: Active Surveillance vs Surgery for Low-Risk Papillary
Active surveillance for low-risk papillary thyroid microcarcinoma has demonstrated oncologic safety comparable to immediate surgery in landmark Japanese trials. This review covers patient selection criteria, monitoring protocols, and triggers for delayed surgical intervention.

Heart Valve Disease: TAVR Expansion to Lower-Risk and Younger Patients
Transcatheter aortic valve replacement has expanded from prohibitive-risk to low-risk patients within a decade. This review covers the PARTNER 3 and Evolut Low Risk trial data, durability concerns, lifetime management considerations for younger patients, and evolving indications for transcatheter mitral and tricuspid interventions.

Migraine Acute Treatment: Gepants, Ditans, and Triptan Comparison
CGRP receptor antagonists (gepants) and 5-HT1F agonists (ditans) have expanded acute migraine pharmacotherapy beyond triptans for the first time in decades. This review compares efficacy, tolerability, and positioning of these drug classes with practical prescribing guidance.

Aortic Stenosis Severity Assessment: Echo Parameters and Decision Timing
Echocardiographic grading of aortic stenosis relies on aortic valve area, mean gradient, and peak velocity, but discordant findings occur in up to 30% of cases. This review covers current severity classification, low-flow low-gradient subtypes, and optimal timing for surgical or transcatheter intervention.
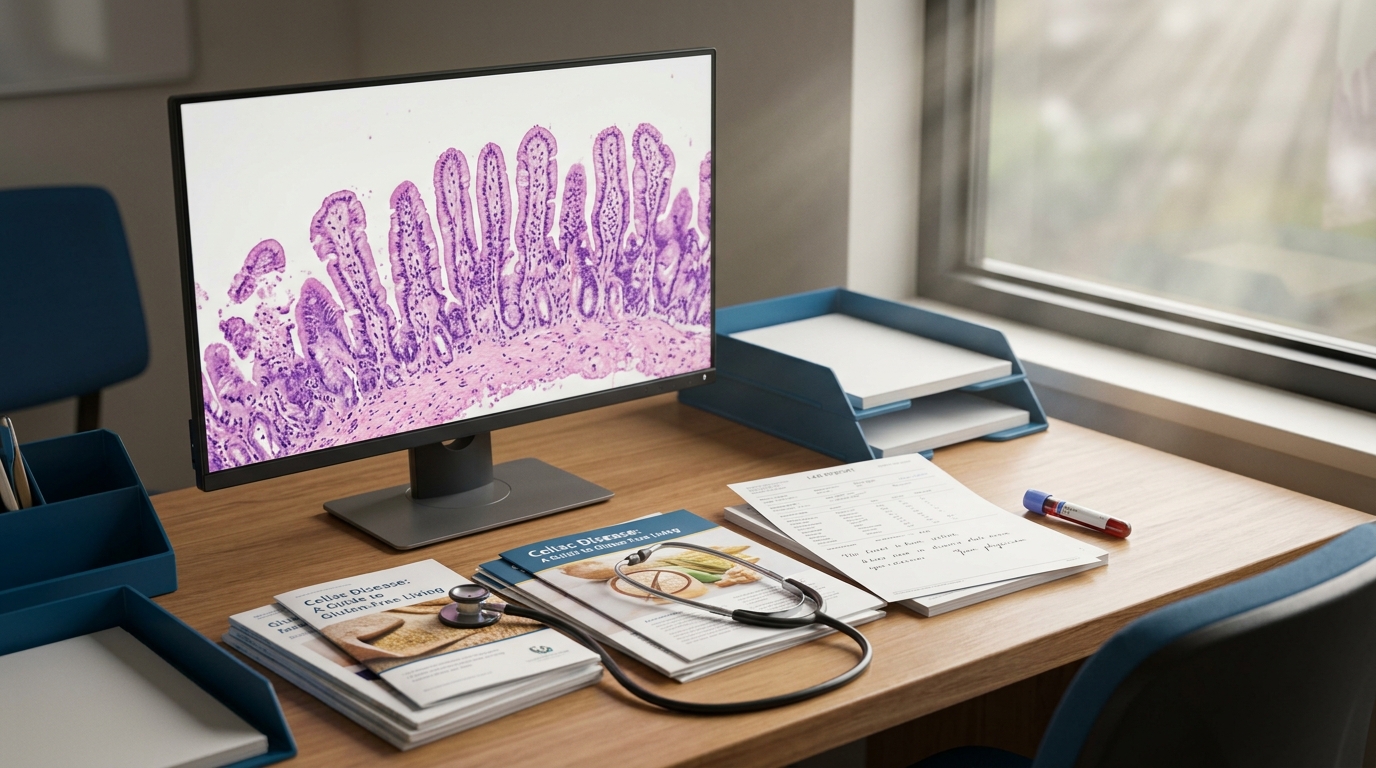
Celiac Disease Diagnosis: Serology, Biopsy, and Gluten-Free Management
Celiac disease affects approximately 1% of the population but remains underdiagnosed by a factor of 3-5. Current diagnostic algorithms combine tissue transglutaminase antibodies with duodenal biopsy, though emerging evidence supports serology-only diagnosis in select populations.

Bipolar Disorder Pharmacotherapy: Lithium, Valproate, and Atypical Antipsychotics
Mood stabilizer selection in bipolar disorder depends on episode polarity, comorbidities, and patient-specific risk factors. This review compares lithium, valproate, and atypical antipsychotics across acute mania, bipolar depression, and maintenance phases with trial-level evidence.

Diabetic Retinopathy Screening: AI-Assisted Imaging and Referral Criteria
Diabetic retinopathy remains the leading cause of blindness among working-age adults. AI-based retinal screening systems now achieve sensitivity exceeding 90% for referable disease, enabling point-of-care screening in primary care settings with immediate results.

Acute Pancreatitis Management: Fluid Resuscitation and Nutrition Timing
Acute pancreatitis management has shifted significantly in the past five years, with goal-directed fluid resuscitation replacing aggressive hydration and early oral feeding supplanting prolonged fasting. This review covers the WATERFALL trial, nutrition strategies, and severity-stratified management.

Melanoma Staging and Treatment: Immunotherapy and Targeted Therapy
The 5-year survival rate for metastatic melanoma has improved from 5% to over 50% with immunotherapy and targeted therapy. Current treatment selection depends on BRAF mutation status, disease stage, and patient performance status, with adjuvant and neoadjuvant approaches expanding rapidly.
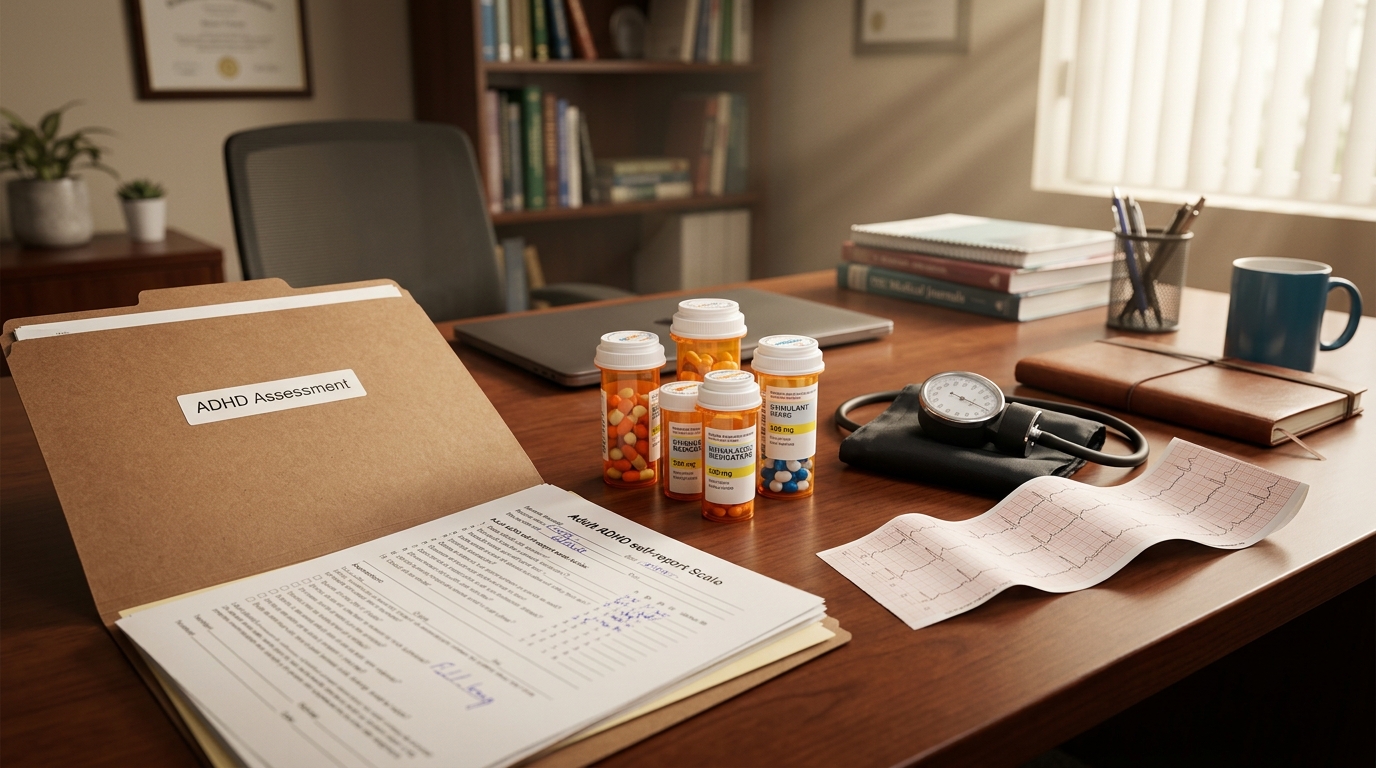
ADHD in Adults: Diagnosis, Stimulant Selection, and Cardiovascular Monitoring
Adult ADHD affects 4-5% of adults and is increasingly diagnosed in primary care. This review covers validated diagnostic instruments, evidence-based pharmacotherapy selection between methylphenidate and amphetamine formulations, and cardiovascular safety monitoring requirements.
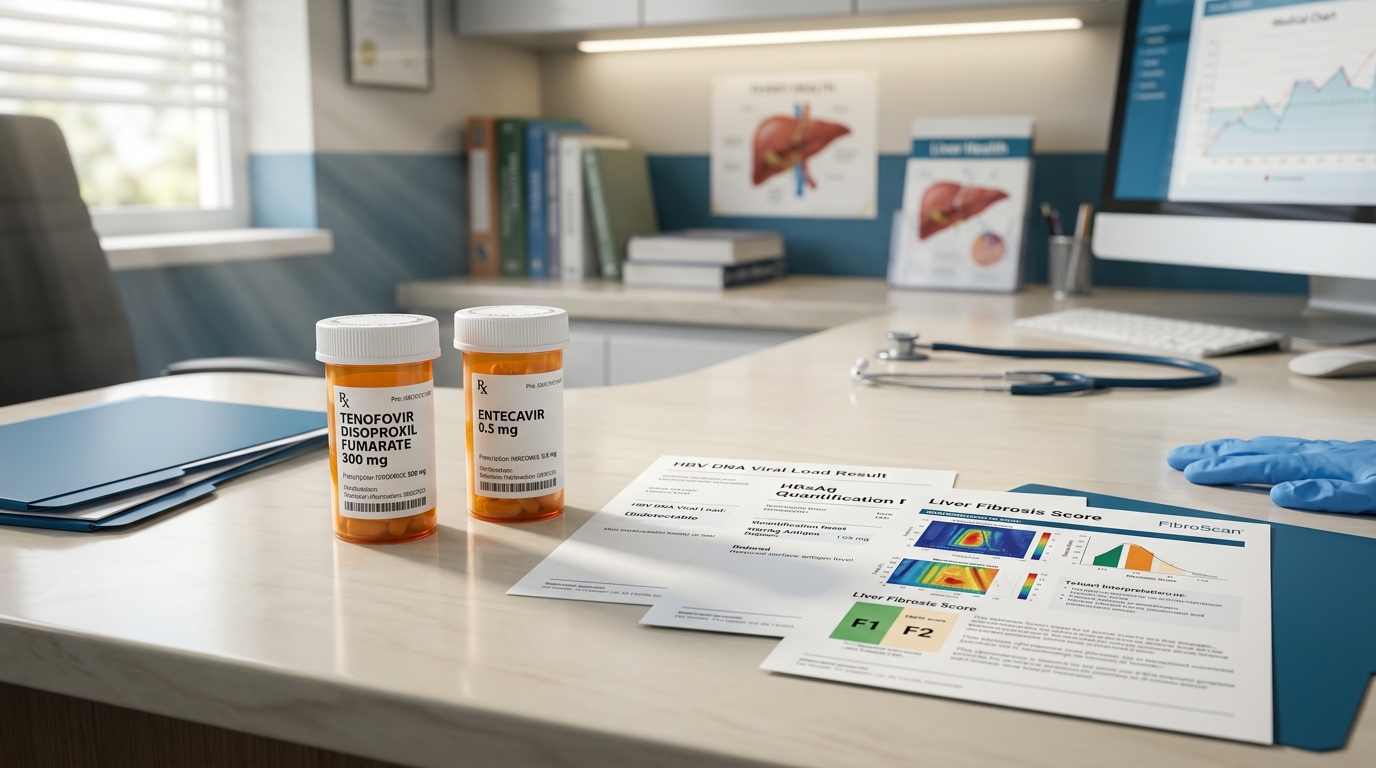
Chronic Hepatitis B: Tenofovir, Entecavir, and Functional Cure Strategies
Approximately 296 million people worldwide have chronic hepatitis B infection. First-line nucleos(t)ide analog therapy with tenofovir or entecavir achieves viral suppression in over 95% of patients, while functional cure strategies targeting HBsAg loss represent the next therapeutic frontier.
Bone Health in Premenopausal Women: When to Screen and How to Treat
Osteoporosis in premenopausal women is uncommon but clinically significant when present, requiring a fundamentally different diagnostic and therapeutic approach than in postmenopausal patients. This review covers appropriate indications for DXA screening, secondary cause evaluation, and treatment options.

Pediatric Obesity: GLP-1 Agonist Approval and Multidisciplinary Management
Pediatric obesity now affects 19.7% of US children and adolescents. FDA approval of semaglutide and liraglutide for adolescents has expanded pharmacotherapy options, but optimal outcomes require integration with intensive behavioral and dietary interventions.

Endometriosis Management: Hormonal Therapy and Surgical Decision-Making
Endometriosis affects approximately 10% of reproductive-age women, with an average diagnostic delay of 7-10 years. This review covers empiric hormonal therapy, imaging advances, and evidence-based surgical approaches for pelvic pain and infertility.

Polycystic Ovary Syndrome: Metabolic Risk and Treatment Algorithm
PCOS affects 8-13% of reproductive-age women and is the most common cause of anovulatory infertility. The 2023 International Evidence-Based Guideline updates diagnostic criteria and emphasizes metabolic risk assessment as a cornerstone of management.
Parkinson's Disease: Levodopa Optimization and Adjunctive Therapies
Motor fluctuations develop in approximately 50% of Parkinson's disease patients within 5 years of levodopa initiation. This review covers optimal levodopa dosing strategies, adjunctive therapy selection, and emerging device-based interventions for motor and non-motor symptoms.

Chronic Cough Evaluation: A Systematic Diagnostic Approach
Chronic cough, defined as cough persisting beyond 8 weeks, affects 10-12% of the general population. A systematic algorithm targeting the three most common etiologies (upper airway cough syndrome, asthma, and GERD) resolves 85-95% of cases when applied rigorously.

Iron Deficiency Anemia: IV Iron Formulations and Indications
Iron deficiency is the most common nutritional deficiency worldwide, affecting an estimated 1.2 billion people. Intravenous iron formulations now allow complete repletion in 1-2 infusions, fundamentally changing management for patients with malabsorption, intolerance to oral iron, or ongoing losses.

Cervical Cancer Screening: HPV Primary Testing and Updated Intervals
Cervical cancer screening guidelines now endorse HPV primary testing as a preferred strategy for women aged 25-65. Extended screening intervals of 5 years with HPV testing alone or co-testing improve detection of high-grade lesions while reducing unnecessary colposcopy.

Benign Prostatic Hyperplasia: Medical Therapy Comparison and Surgical Options
BPH affects 50% of men by age 60 and 90% by age 85. Alpha-blockers, 5-alpha reductase inhibitors, and combination therapy provide effective medical management, while minimally invasive surgical therapies offer durable alternatives with favorable risk profiles.

Obesity Pharmacotherapy: Semaglutide, Tirzepatide, and Combination Approaches
The obesity pharmacotherapy landscape has been transformed by GLP-1 and dual GLP-1/GIP receptor agonists achieving 15-25% total body weight loss. This review compares approved agents, emerging combination therapies, and evidence-based patient selection criteria.

Myasthenia Gravis: FcRn Inhibitors and Complement-Directed Therapies
The myasthenia gravis treatment landscape has been revolutionized by targeted therapies, with FcRn inhibitors and complement inhibitors achieving rapid, clinically meaningful improvement in generalized disease. These agents offer new options for refractory patients and may reshape the treatment paradigm.

Status Epilepticus: Updated Treatment Algorithm and Refractory Management
Status epilepticus carries a mortality rate of 10-30% and requires a time-critical, protocolized approach. The ESETT trial has standardized second-line therapy selection, while emerging evidence guides management of refractory and super-refractory cases.

Chronic Kidney Disease-Mineral Bone Disorder: Phosphate Management
CKD-mineral and bone disorder (CKD-MBD) begins early in CKD and drives cardiovascular calcification and fracture risk. Phosphate management, guided by the 2024 KDIGO update, integrates dietary modification, phosphate binders, and novel therapies targeting FGF23 and the phosphate-kidney axis.

Inflammatory Arthritis Differential: RA vs PsA vs SpA Clinical Features
Distinguishing rheumatoid arthritis from psoriatic arthritis and spondyloarthritis is essential for targeted therapy selection. This review compares clinical patterns, serologic markers, imaging findings, and classification criteria across these three inflammatory arthritides.

Neonatal Sepsis: Early vs Late Onset and Empiric Antibiotic Selection
Neonatal sepsis remains a leading cause of morbidity and mortality in the NICU, with early-onset sepsis occurring within 72 hours and late-onset sepsis after 72 hours of life. This review covers risk stratification tools, empiric antibiotic regimens, and evidence for antibiotic duration.

Concussion Management: Return-to-Play Protocols and Persistent Symptoms
Sport-related concussion management has evolved significantly with the 2023 Amsterdam Consensus Statement. Current protocols emphasize individualized recovery timelines, graduated return-to-play progression, and evidence-based management of persistent post-concussion symptoms.
Hereditary Cancer Syndromes: When to Test and Surveillance Guidelines
Hereditary cancer syndromes account for 5-10% of all cancers. Expanded multigene panel testing has identified at-risk individuals earlier, but appropriate patient selection, variant interpretation, and risk-stratified surveillance protocols remain essential for clinical benefit.
Contrast-Induced Nephropathy: Prevention Strategies and Risk Assessment
The risk of contrast-induced nephropathy has been overstated in historical literature, with contemporary evidence suggesting true incidence is significantly lower than previously reported. This review covers updated risk stratification, evidence-based prevention strategies, and guideline recommendations.

Polypharmacy in Elderly Patients: An Evidence-Based Deprescribing Framework
Your 82-year-old patient takes twelve medications. Each one was individually appropriate when prescribed. The problem is not any single drug — it is the cumulative burden of all of them in an aging body. Here is a structured approach to deciding what to stop, and in what order.

Free Clinical Tools Every Physician Should Know About in 2026
The landscape of free clinical tools has expanded significantly. Here is a practical overview of what is available at no cost for point-of-care reference, evidence synthesis, drug interactions, and more.

GLP-1 Receptor Agonists Beyond Diabetes: Cardiovascular and Renal Evidence
SELECT proved semaglutide cuts MACE in patients without diabetes. FLOW stopped early because semaglutide slowed CKD progression that dramatically. Here is what the trials actually show, and what they mean for the patient in your office tomorrow.
How to Verify Medical Citations: A Step-by-Step Guide
A practical, step-by-step guide for physicians to verify whether a medical citation is real, accurate, and correctly attributed — whether it comes from a clinical tool, a colleague, or a published review.
Understanding Preprint Evidence: What Clinicians Need to Know
One-third of practicing physicians have used a preprint to inform a clinical decision. One preprint — dexamethasone in severe COVID — saved thousands of lives by bypassing the publication timeline. Another — hydroxychloroquine — caused widespread harm. The format is neutral. The quality of the science is what matters.
Beyond Traditional Medical References: The Evolution of Clinical Decision Support
From textbooks to UpToDate to search-based tools to clinical intelligence platforms — each generation solved problems the last could not. Here is what changed and why it matters.

Interpreting Elevated hs-CRP in the Context of Multiple Comorbidities
Your 64-year-old patient has an hs-CRP of 8.2 and carries five diagnoses that all cause inflammation. The CRP is elevated. By which condition? All of them? Or something new you have not found yet?
Why Clinical AI Tools Hallucinate Citations — And How to Verify Them
A colleague asked me to check a citation from an AI clinical summary. The paper it referenced — a 2023 Lancet meta-analysis — did not exist. The authors were real. The journal was real. The study was fabricated. Studies show this happens up to 47% of the time.

The Complete Guide to Clinical Decision Support in 2026
A definitive guide to clinical decision support tools in 2026 — covering the history, current landscape, evaluation criteria, citation verification, cross-system reasoning, and future directions of CDS technology for physicians.
Can Physicians Trust Clinical Intelligence Tools? An Evidence-Based Framework
Physician trust in clinical tools should be earned through transparency, verification, and evidence — not marketing. Here is a framework for evaluating whether a clinical intelligence tool deserves your trust.

Clinical Citation Verification: A Comprehensive Guide for Healthcare Professionals
Why clinical citations hallucinate, the types of hallucinations that matter most, and how verification systems work. A comprehensive guide for any healthcare professional relying on evidence-based tools.

Tools for Complex Multi-System Cases: What Physicians Need
Complex multi-system cases challenge traditional clinical tools because the answer lives at the intersection of specialties. Here is why these cases are hard, what an ideal tool would do, and what the evidence shows.

Drug-Nutrient Interactions Physicians Miss: A Cross-System Review
Your patient on metformin, furosemide, omeprazole, escitalopram, and atorvastatin faces simultaneous depletion of B12, magnesium, thiamine, calcium, sodium, and CoQ10. No EHR alert will fire for this pattern. Nobody owns it.
The Gut-Brain Axis: Clinical Evidence for Psychiatric Practice
The microbiome-mood connection is real and biologically plausible. But in 2026, the clinical implications are more modest than the headlines suggest: dietary counseling has good adjunctive evidence, specific probiotic strains show small effects, and GI comorbidity screening should be standard. Here is what the data actually support.
Cross-System Clinical Reasoning: Why No Single Specialty Has the Full Picture
Cross-system clinical reasoning connects evidence across organ systems and specialties to reveal diagnoses and treatment strategies that no single specialty perspective would identify. Here is why it matters, with detailed case examples.
Beyond Single-Specialty Answers: Why Cross-System Reasoning Matters
A 58-year-old with type 2 diabetes, eGFR 38, and new atrial fibrillation needs anticoagulation. The cardiology answer, the nephrology answer, and the endocrinology answer are three different answers. Your patient needs one.
Evidence-Based Medicine in the Age of Information Overload: A Physician's Survival Guide
With 1.5 million new medical articles published annually, staying current with evidence-based medicine is impossible through traditional methods. A practical guide for managing medical information overload without compromising patient care.

Patient-Specific Evidence: Why Subgroup Data Changes Clinical Decisions
Overall trial results often mask clinically important differences between patient subgroups. Understanding when and how subgroup data changes the decision is essential for truly personalized evidence-based medicine.

Shared Decision-Making with Complex Evidence: A Practical Guide
Shared decision-making works best when the evidence is clear. It matters most when the evidence is not. Here is a framework for communicating NNT, NNH, uncertainty, and conflicting data to patients who need to make real decisions.
When Depression Doesn't Respond to SSRIs: A Cross-System Differential
Before you add an atypical antipsychotic to that SSRI, check the thyroid, the B12, the CRP, and the sleep study. A structured cross-system evaluation reveals treatable causes in up to 40% of cases labeled treatment-resistant.

What to Look for in a Clinical Decision Support Tool in 2026
Five years ago, clinical decision support meant UpToDate. The landscape in 2026 looks different. Here is a framework for evaluating tools based on what actually matters when you are standing in front of a patient.
SGLT2 Inhibitors in HFpEF with CKD: What the Evidence Shows
A 72-year-old with HFpEF, eGFR 34, type 2 diabetes, and a recent heart failure hospitalization. Should she start an SGLT2 inhibitor? The answer spans three trial programs, and the data are clearer than you might expect.

The Bench-to-Bedside Gap: Why Evidence Takes 17 Years to Reach Patients
SGLT2 inhibitors have a Class I recommendation for heart failure. Only 13% of eligible patients are on one. The gap between what the evidence shows and what patients receive is measured in decades and tens of thousands of lives. Here is where the years go.
Showing 1–100 of 100 articles